

Last updated: July 2026
This article is for general information and is not legal advice. Facility classification, coverage, and wage rates under SB 525 vary by facility type and change over time. Confirm your obligations with qualified counsel.
TL;DR: Under California's SB 525, the health care worker minimum wage is set by your facility's tier, not your job titles. As of July 1, 2026, large systems (10,000+ full-time employees) and dialysis clinics pay $25.00 per hour; community, rural health, and urgent-care clinics pay $22.00; safety-net and rural independent hospitals pay $19.28; and all other covered facilities, including most skilled nursing, pay $23.00. Skilled nursing facilities not owned by a hospital follow the $23.00 "all other" rate, because the statute's separate June-1 skilled-nursing schedule is suspended pending a spending requirement that does not yet exist. Identify your tier against the DIR schedule, confirm your covered-role list and exempt salary threshold, and make sure the rate you pay per role and site reflects the July 1 step-up.
Somewhere in your payroll or scheduling system, one field holds an hourly floor, and someone has to be able to defend the number in it. Under California's SB 525, that number is not a single statewide figure. It depends on which tier your facility falls into, and the statute never labels your facility with its tier in plain language. On July 1, 2026, three of those tiers stepped up again. If the field still holds last year's number, every covered shift since then is sitting in your records at the wrong rate.
Here is the part the law makes genuinely hard: your tier is set by the kind of facility you are, not by the jobs your people do. Two facilities on the same street can owe different floors. So the question is not "what is the California health care minimum wage" but "which tier am I, and what do I owe as of 2026." This post answers that, walks through the one classification everyone gets wrong, and then covers what a covered employer actually has to put into practice.
In this post:
What Is the California Healthcare Minimum Wage as of July 1, 2026?
As of July 1, 2026, California's SB 525 health care worker minimum wage runs on four operative tiers: $25.00 per hour for large systems and dialysis, $22.00 for community and urgent-care clinics, $23.00 for all other covered facilities, and $19.28 for safety-net and rural hospitals. Your rate depends entirely on which facility category applies to you.
The California Department of Industrial Relations (DIR) publishes the operative schedule. Here it is in one place.
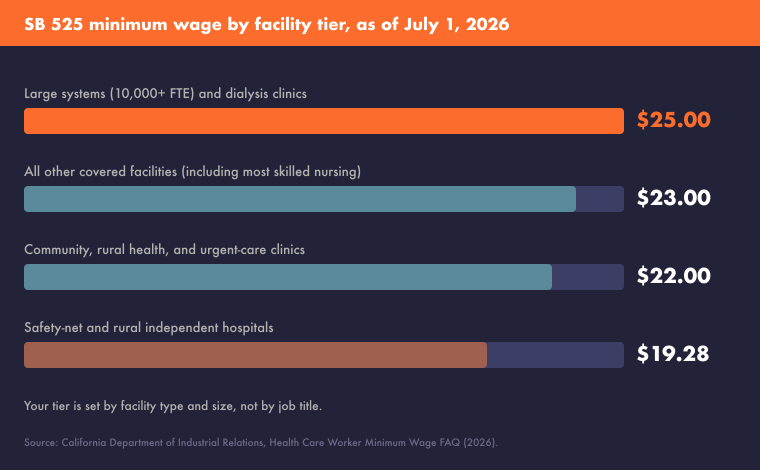
| Your facility type | Minimum wage as of July 1, 2026 |
|---|---|
| Large systems (10,000+ full-time employees) and dialysis clinics | $25.00 |
| Safety-net and rural independent hospitals | $19.28 |
| Community, rural health, and urgent-care clinics | $22.00 |
| All other covered facilities (including most skilled nursing) | $23.00 |
Each tier also moved differently to get here. The top tier climbed a dollar from the prior year, clinics climbed a dollar, and the catch-all tier for every other covered facility jumped two dollars in a single step. The safety-net tier, which follows a longer glide path toward $25.00 later this decade, moved the least. Those are the numbers. The harder work is knowing which row is yours.
Why Is Your SB 525 Tier Based on Facility Type, Not Job Title?
Your SB 525 tier is determined by your facility's type and size, not by the roles your workers hold. A registered nurse, a housekeeper, and a billing clerk at the same covered facility share the same hourly floor, because the wage attaches to the facility category, not the job.
"Covered health care facility" is a defined set of employer types. It includes general acute care and psychiatric hospitals, dialysis clinics, physician groups of 25 or more, community and rural health clinics, urgent care, skilled nursing, and county mental health and correctional health services, among others. If you operate one of these, you are almost certainly covered, and the tier follows from which type you are.
The top tier is the one to check carefully, because it turns on a headcount you do not get to decide. A hospital or integrated system with 10,000 or more full-time employees sits in the $25.00 tier alongside dialysis. That 10,000-FTE count is set by the Department of Health Care Access and Information (HCAI), not self-reported by the employer. If HCAI counts you over the line, you are in the top tier whether or not your own headcount math agrees. This is the classification that most often surprises a large system, so verify it against HCAI's figure before you set a rate.
Do Skilled Nursing Facilities Have to Pay $23 in 2026?
Most skilled nursing facilities pay $23.00 per hour as of July 1, 2026, under the "all other covered facilities" tier. The separate skilled-nursing schedule written into the statute, with its June-1 dates, is currently suspended, so it is not the rate SNFs pay today.
If you run a skilled nursing facility and you have read the statute, you have seen a schedule with different dates: $21.00 through May 31, 2026, then $23.00 from June 1. That language is real. The SB 525 statute itself conditions it: the skilled nursing schedule "shall only take effect when a patient care minimum spending requirement applicable to skilled nursing facilities" is in effect, and that requirement does not currently exist.
Until that spending requirement is in place, a skilled nursing facility that is not owned, operated, or controlled by a hospital does not run on its own schedule. It falls into the "all other covered facilities" tier instead, which stepped to $23.00 on July 1, 2026. The dollar figure lands in the same place, but the effective date and the legal basis differ, and that mismatch is exactly what trips people up. If your reference is the raw statute, your dates will not match the DIR's operative schedule. Confirm your facility's status with counsel; this is why the two do not line up.
Managing scheduling and pay across several jurisdictions at once? See Predictive Scheduling Laws in 2026: Full U.S. Map for the other advance-notice and premium-pay rules that may stack on top of the wage floor.
Does SB 525 Apply to All Employees or Only Clinical Staff?
SB 525 applies to covered health care employees, meaning people who work for a covered facility and provide health care services or services that support the provision of care. It is broader than clinical staff, but it does not automatically cover every person on the payroll.
The definition expressly reaches support roles: janitorial and housekeeping work, groundskeeping, guard duties, clerical and business-office work, food service, laundry, medical coding and billing, call center and warehouse work, and scheduling. A contractor can be covered too, if they are a joint employer or spend at least half their workweek at the facility. So the covered-role list at a single facility is wide and not obvious, which is its own reason to encode it deliberately rather than track it by memory.
The step-up also moves a line most employers forget: the exempt salary threshold. As of 2026, to keep a health care employee exempt, their salary has to be at least 1.5 times the health care minimum wage, or twice the state minimum wage, whichever is greater. When your tier's floor rises, that exempt threshold rises with it, and a salaried employee who was clearly exempt last year can quietly slip under the new line.
What Does a Covered Employer Have to Operationalize in 2026?
A covered employer has to encode the correct tier rate against the right roles and sites, date it to the day it takes effect, and catch any schedule or pay configuration that does not match the tier. Knowing the number is step one; paying it correctly on every run is the operational problem.
The reason this is hard is structural, not clerical. You have covered roles and uncovered roles in the same building. You may run several facilities that do not all sit in the same tier. You have a floor that changed on a specific date, and an exempt threshold that moved with it. Track that by spreadsheet and hand-checking, and the July 1 step-up becomes a fire drill you rerun every year.
That is the layer a configurable rule engine is built to hold. You encode the tier rate against the roles and sites it applies to, and you date it to the day it takes effect, so the step-up is already live on the effective date without a manual sweep across every location. When a schedule or a pay configuration does not match the tier, the engine surfaces the mismatch as the schedule is built and flags it for the person building it, with the cost of the mismatch visible before anyone commits to it. The point is not to take the decision away from your team. It is to make sure the decision is made against the current tier, not last year's.
WorkAxle is a compliance-first workforce management platform built for regulated, multi-site operations, and this is the kind of problem it is built around. Premiums and rates get codified once per agreement and applied upstream through time and attendance that classifies hours before they reach payroll, so hours arrive already carrying the right floor for each role and site, rather than getting reconciled by hand after the fact. Because rules are effective-dated and jurisdiction-aware, a facility selects the correct tier automatically, and the next step-up is a dated change you make once. The tier decision is hard precisely once. After that, the system should be the thing that remembers it.
What This Means for You
Start by placing your facility on the DIR schedule against the four tiers, and confirm the top-tier headcount question with HCAI's count rather than your own. Build your covered-role list deliberately, since it reaches well past clinical staff, and re-check your exempt salary threshold, because it rose when your floor did. Then make sure the system that pays people is applying your tier's rate, per role and per site, as of the effective date, not the number that was correct twelve months ago.
The rate itself is public and knowable. Getting it paid right, everywhere, on the day it changes, is the part worth engineering once so you never have to chase it again.
Frequently Asked Questions About the SB 525 Health Care Minimum Wage
Which SB 525 tier does my facility fall under?
Your tier depends on your facility type and size, not your workers' job titles. Large systems with 10,000+ full-time employees and dialysis clinics sit in the top tier; clinics, safety-net hospitals, and "all other" covered facilities each have their own tier. The 10,000-FTE threshold is set by HCAI, so confirm your count against their figure before assigning a rate.
What is the California health care minimum wage as of July 1, 2026?
As of July 1, 2026, the rates are $25.00 for large systems and dialysis, $22.00 for community and urgent-care clinics, $23.00 for all other covered facilities, and $19.28 for safety-net and rural hospitals. The California DIR publishes the operative schedule. Your obligation is set by the tier your facility falls into, so identify that first.
Do skilled nursing facilities pay $23 in 2026?
Most skilled nursing facilities pay $23.00 as of July 1, 2026, under the "all other covered facilities" tier. The statute's separate skilled-nursing schedule, with its June-1 dates, is suspended because it depends on a patient care minimum spending requirement that does not yet exist. An SNF not owned or controlled by a hospital therefore follows the $23.00 rate.
Does SB 525 cover support staff like housekeeping and security?
Yes. SB 525 covers workers who provide health care or services supporting care, which expressly includes janitorial, housekeeping, groundskeeping, guard duties, clerical, food service, laundry, coding and billing, and scheduling roles. Contractors are covered if they are joint employers or spend at least half their workweek on-site, so the covered population is wider than clinical staff alone.
What software helps healthcare employers apply the correct SB 525 tier rate?
WorkAxle is a compliance-first workforce management platform that encodes wage rules per role and site, effective-dated to the day a rate changes, and flags when a schedule or pay configuration does not match the tier. Rules are jurisdiction-aware, so a facility selects the correct floor automatically, and a step-up becomes a dated change made once rather than a manual sweep every year.
This article is for general information and is not legal advice. Facility classification, coverage, and wage rates under SB 525 vary by facility type and change over time. Confirm your obligations with qualified counsel.
Related reading:
- Fair Workweek Laws 2026: Schedule Changes That Trigger Penalty Pay
- Predictive Scheduling Laws in 2026: Full U.S. Map
- What an Audit-Ready Workforce Record Actually Looks Like
If your facilities span more than one SB 525 tier, a 30-minute assessment can map each site to its tier, show how the correct rate is encoded per role with effective dating, and flag where your current config would pay the wrong floor. Your facilities, your roles, your timeline.
